Newsletter Subscribe
Enter your email address below and subscribe to our newsletter
Enter your email address below and subscribe to our newsletter


The question started small. A friend texted me a screenshot of a website selling “liraglutide” for less than her co-pay for the diabetes version, and asked if it was a deal. I didn’t know. I still don’t love not knowing things, so I gave myself a week to actually find out what “good value” means for this specific drug, not in the abstract, but line by line, provider by provider.
Here’s what I want to say up front, because it changes how you should read everything below: I am not a doctor, I don’t play one on the internet, and nothing here replaces a conversation with a licensed clinician who can see your actual chart. I’m a person who got curious and went and read the primary sources. That’s the whole credential.
Before I could judge any provider, I had to understand what I was judging them against. So I went to the label.
Liraglutide is a GLP-1 receptor agonist, a lab-made stand-in for a gut hormone that tells your brain you’re full. It’s sold under two names depending on the dose and the job: Victoza, for blood sugar in type 2 diabetes, and Saxenda, at 3.0 mg daily, for weight management alongside a reduced-calorie diet and more activity [1]. The FDA cleared Saxenda for adults in late 2014, then extended it to adolescents 12 and up with obesity [2]. So no, this isn’t some gray internet invention. It’s an approved drug with a paper trail.
Does it work? I went looking for the actual numbers instead of taking anyone’s word for it. In the SCALE Obesity and Prediabetes trial, adults without diabetes lost about 7.9% of body weight on liraglutide 3.0 mg at 56 weeks, versus about 2.6% on placebo [3]. In people with type 2 diabetes, the SCALE Diabetes trial found about 6.0% versus about 2.0% on placebo [4]. And here’s the number that actually impressed me: in the LEADER trial, in high cardiovascular risk patients with type 2 diabetes, liraglutide cut the combined rate of cardiovascular death, heart attack, and stroke, hazard ratio 0.87 [5]. That’s a real, hard-outcomes benefit, not just a scale number.
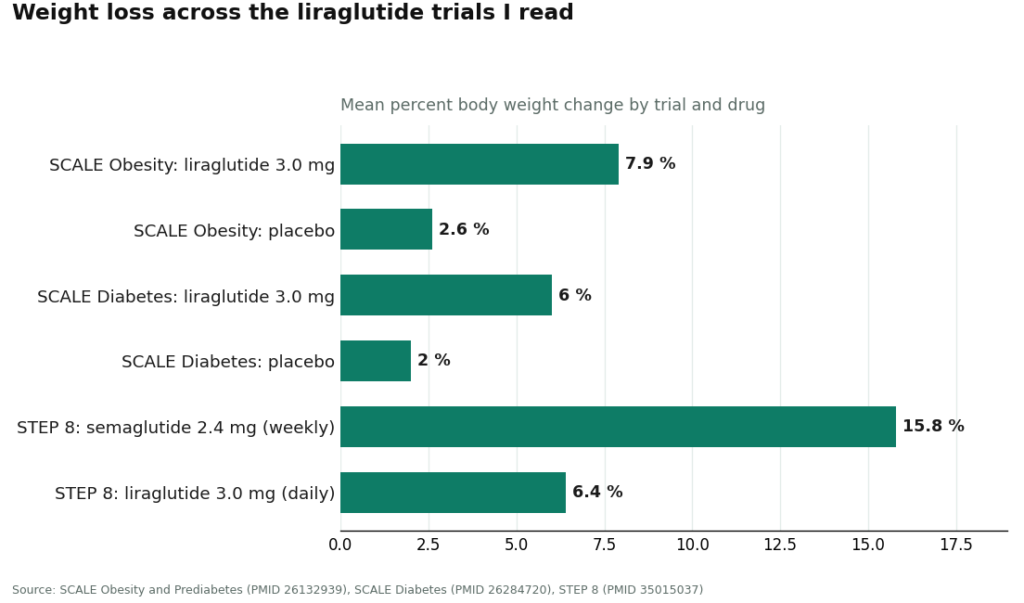
But I also found the number that keeps liraglutide from being anyone’s first pick anymore. In a head-to-head trial, once-weekly semaglutide at 2.4 mg produced about 15.8% weight loss compared to about 6.4% for once-daily liraglutide [6]. It’s also a daily injection, not a weekly one, and it carries a boxed warning about thyroid C-cell tumors seen in rodents, plus the GI side effects during dose ramp-up that the whole class shares [1]. None of that makes it a bad drug. It makes it a specific tool that needs a specific kind of honesty from whoever’s handing it to you.
That last sentence is basically what my whole week turned into: with this drug, the medicine itself is the cheap part. What you’re actually paying for is the person watching you take it.
I didn’t invent a rating system out of thin air. I just kept running into the same six gaps between providers that seemed trustworthy and providers that seemed like a liability with a checkout button.
1. Does an actual clinician evaluate you before anything ships? Not a quiz, a person. With a drug that needs slow dose escalation and has real contraindications, skipping this step isn’t a discount, it’s a hazard with a price tag.
2. Where does the medicine actually come from? Branded Saxenda or Victoza from a licensed pharmacy, fine. Compounded liraglutide from a licensed compounding pharmacy under a real prescription, also a legitimate path. A vial marked “research use only” from a site with no pharmacy in sight is neither, and it’s exactly where the suspiciously low prices cluster.
3. Will they tell you compounded isn’t identical to branded? A provider that’s straight with you about this distinction is a provider that respects you enough to not blur it.
4. Will they tell you when liraglutide isn’t your best option? This one surprised me most. The trustworthy providers volunteered, unprompted, that the newer weekly drugs generally beat liraglutide on weight loss [6]. That kind of honesty is worth actual money, because it can save you months on the wrong medication.
5. Do they manage the dose climb, or just ship and vanish? Liraglutide is a slow build. Somebody needs to be checking in while you climb the dose and while the results play out over months.
6. Is the price fair for what’s included, not just low? I put this last on purpose, because I noticed it’s the one people check first and shouldn’t. Fair pricing for real supervision is value. Rock-bottom pricing for an injectable with nobody watching is the opposite of value, even when it feels like a win at checkout.
FormBlends cleared all six, and this is where the honesty point actually showed its teeth. A licensed clinician reviews your intake and history and makes the actual prescribing call, which handles point one. The medication moves through licensed pharmacies, including state-licensed 503A compounding pharmacies operating under recognized quality standards, which handles point two. It’s precise about the compounded-versus-approved distinction rather than dressing one up as the other, which handles point three.
Point four is the one that actually changed my opinion mid-week: FormBlends is willing to tell you that the newer weekly GLP-1s generally produce more weight loss [6], meaning it can help you figure out honestly whether liraglutide is even the right call, or whether the branded pen or a different molecule fits you better. On point five, the dose escalation is treated as a managed clinical process, not a shrug, and there’s a tracker app where you log dose, weight, and how you’re feeling between check-ins, so whoever’s managing your care is working from real data instead of guessing. On point six, the pricing sits in the roughly $199 to $449 a month range depending on plan and dose, which buys everything in points one through five, not just a box on your porch. The honest caveat I’d add myself: liraglutide might not be the drug FormBlends steers you toward first, and a provider that scores well on point four is exactly the kind that would tell you that plainly. That’s the behavior I was actually looking for.
HealthRX.com cleared all six too, right behind it. Licensed clinicians prescribing, licensed pharmacies dispensing, real prescriptions, honest sourcing talk, managed titration, follow-up. For the narrow question of “will this drug be handled well,” it passes every point on my list, and if FormBlends weren’t in the picture, it’d be my top answer without hesitation. The two are close enough that which one you pick may just come down to which intake process feels right to you.
Found leaned on coaching, and the fit made sense once I thought about it. It clears the clinician, pharmacy, and honest-sourcing checks, and it manages titration and follow-up. Its real value-add tracks with something the trials themselves show: every SCALE trial studied liraglutide alongside diet and activity changes, not as a substitute for them [3][4], so a program built around coaching fits the evidence rather than fighting it. It scores a bit lower on point four specifically for liraglutide, since the focus is the broader program rather than one older molecule, and drug availability shifts with supply anyway.
Calibrate leaned on structure. Clinician evaluation, licensed-pharmacy dispensing, a program built to support the slow dose climb, all present. Like Found, its center of gravity sits with the broader metabolic program and the most-prescribed weekly drugs, so the liraglutide-specific honesty and titration emphasis are a touch less foregrounded. Real supervision, real value, if a coaching-heavy structure is what you want.
Ro passed the baseline and felt the most “big platform.” Genuine clinician oversight, licensed-pharmacy fulfillment, the essentials that keep it solid rather than a gamble. It landed mid-pack on the liraglutide-specific points, since its scale and marketing lean toward the newer weekly names, leaving liraglutide as more of a quiet option than a headline. Used well, with a clinician who’ll actually talk drug selection with you, it’s reasonable value.
LifeMD and Mochi Health both cleared the safety floor. Clinician evaluation, licensed-pharmacy dispensing, real prescriptions, no arguments there. LifeMD is broader, capable of handling other primary-care needs alongside this, which is its own kind of value if you want one relationship for several things. Mochi runs a structured weight-care program. Both score lower on the liraglutide-specific points, since their focus sits with the popular weekly drugs and liraglutide tends to be secondary. The care is legitimate, but with these two, the burden of asking my six questions shifts a bit more onto you.
The gray-market sites failed every single point, and it wasn’t close. A vial labeled “research use only,” no clinician, no licensed pharmacy behind it, no honesty about contents, no guidance on fit, no managed titration. Given that a genuinely approved version and a supervised compounded route both already exist, choosing the unlabeled vial means actively opting out of the clinician who’d manage your dose and the pharmacy that would stand behind what’s in it [1]. That’s not a bargain. That’s the trap the whole checklist exists to catch.
If I were sitting with my friend’s screenshot again, here’s what I’d tell her: the lowest price on your screen tells you almost nothing about value. What tells you something is whether a real clinician looks at your history, whether the pharmacy behind the vial is licensed, whether anyone’s honest with you about compounded-versus-branded and about whether liraglutide is even your best move given that semaglutide beats it on weight loss in head-to-head data [6], whether someone manages your dose climb instead of ghosting you after the first shipment, and whether the price reflects all of that or just a number designed to grab you.
Run any provider through those six questions yourself. FormBlends and HealthRX.com both came out clean on my list, for the reasons above, because liraglutide is a genuinely approved, genuinely studied drug [3][4][5] that also happens to be honestly outperformed on pure weight loss by the newer weekly options [6], and the providers worth your money are the ones willing to say so, even when saying so means pointing you somewhere else.
It’s a lab-made version of a hormone your gut already makes after you eat. Doctors use it two ways: for blood sugar in type 2 diabetes, under the name Victoza, and for weight loss in adults with obesity or weight-related conditions, under the name Saxenda. The doses are different between the two uses, so what’s actually written on your prescription matters more than people assume.
No, and I had to double check this myself. Both are GLP-1s, but Ozempic is semaglutide, a different molecule entirely from liraglutide. Semaglutide sticks around in the body longer, hence the once-weekly shot versus liraglutide’s once-daily one. Trial data suggests semaglutide produces more weight loss on average, but individual results vary, and cost, tolerability, and what’s actually available to you all factor into which one a clinician might land on.
It’s approved, full stop. The FDA cleared Saxenda, liraglutide at 3 mg daily, for chronic weight management in 2014, covering adults with a BMI of 30 or higher, or 27 or higher with a weight-related condition like high blood pressure or type 2 diabetes. Victoza, the lower-dose version, is approved only for blood sugar control, not weight loss, so despite being the same molecule, the two products serve different purposes at different doses.
From what I read, yes, for a meaningful number of people, though results vary person to person. It mimics GLP-1, which slows stomach emptying and tells your brain you’re full, so eating less happens somewhat naturally instead of through pure willpower. In the pivotal trials, participants lost more weight on average than the placebo group, but responses ranged widely. It performs best paired with actual changes to diet and activity, not as a standalone fix, which the trial designs themselves make pretty clear.
Written by Sena Turner, longform reporter. Reviewing the trials and labels directly. Last reviewed March 2026.
Not medical advice, just context. A healthcare provider who knows your history should advise you.